‘Having a Baby is Easier Than Getting a Root Canal’
 By Dr. Anthony Charles Caputo
By Dr. Anthony Charles Caputo
Regardless of your practice, as dentists, we have all heard the jokes and other comments identifying how terrible root canal therapy is for our patients. Despite the advancements in endodontics with respect to efficacy and efficiency in root canal therapy, patients still express their fear of this treatment approach. A study by Matsuura in 1989[i] identified that nearly 66% of systemic complications during dental treatment occur during extraction of teeth and root canal treatment. Interestingly, a recent report in the ADA Morning Huddle discussed an article from TIME Health[ii] that stated “Almost 40% of Americans are more anxious than they were at this time last year, according to a new American Psychiatric Association (APA) poll.” It is not uncommon for a person’s anxiety about personal issues and situations to manifest as increased fear and anxiety when presenting for dental treatment.
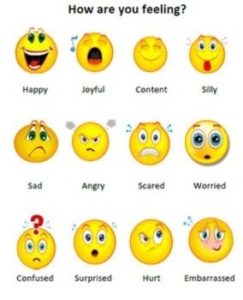
With increased fear and anxiety, it is important to understand and address this situation when a patient presents for endodontic treatment. This needs to be addressed as part of the initial evaluation of the patient. This includes completion and review of the medical history, collection of vital signs (minimally height, weight, blood pressure and pulse rate). The administration of drugs- local anesthesia or sedatives, requires that we obtain the patient’s weight. Height allows for the calculation of BMI which provides information regarding obesity and cardiovascular health. Following the medical evaluation, an anxiety assessment is completed. This is critical to identify how the patient feels about being in your office for treatment. This can be as simple as a visual analog scale that allows a patient to indicate how they are feeling (Figure 1). With identification of how your patient is feeling, you can begin the conversation about what you can do to help them have a successful appointment. Another key factor in assessing a patient’s fear or anxiety, is understanding the Dual Nature of Pain. The International Association for the Study of Pain (IASP) defines pain as, “An unpleasant sensory and/or emotional experience that is associated with actual or potential tissue damage”[iii] The keywords in this definition are “emotional” and “potential.” It is important to appreciate that pain is an emotional experience that is influenced by the potential for injury. This is often a critical assessment of the patient who presents with anxiety or fear to dental treatment.
Figure 1.
There are various strategies available to address anxiety and fear and we often already incorporate some or many of them in our current practices. Suggestion is a vital patient comfort approach and it involves creating an environment where our patients feel welcome and supported. Helpful and kind staff, a comfortable reception area, empathetic chairside manner are all methods of suggestion for the patient to understand you are going to take care of them in the best possible manner. Diagnosis of the condition with thorough explanation allows the patient to understand their situation and what needs to be done. Information empowers the patient and involves them in the treatment process. Profound local anesthesia administration is the most critical part of this process. Without profound anesthesia, the procedure will likely fail particularly for the anxious patient. This is an important point to understand with respect to sedation. The process of sedation is not a way to overcome the various strategies discussed. Sedation is an adjunct approach to facilitate the successful outcome of treatment. Patient selection and local anesthesia are the two key factors in the success of sedation for your patients.
Focusing on sedation, there are different approaches based on what is permitted by your state dental board. Nitrous Oxide-Oxygen Sedation (N2O-O2) is an excellent option for the mild to moderately anxious patient as well as an effective adjunct to other sedation approaches. Oral conscious sedation (OCS) provides an opportunity to improve sedation outcomes when combined with N2O-O2. Depending on the level of sedation being administered- minimal or moderate- there may be permitting requirements by your state dental board. Intravenous conscious sedation (IVCS) generally provides a broader sedation scope than OCS. Beyond minimal or moderate sedation administered by OCS or IVCS, there may be the opportunity to work with an anesthesia provider to administer deep sedation or general anesthesia.
With OCS, the most common drugs to administer are benzodiazepines which are good sedatives that also provide amnesia. Within this class of drugs, triazolam (Halcion) is a common and effective choice in combination with N2O-O2. Other commonly administered benzodiazepines are diazepam (Valium), alprazolam (Xanax) and lorazepam (Ativan). The caution with selecting an appropriate drug for any procedure is the planned length of time for the procedure and the duration of effect of the drug administered. For this reason, Halcion is an excellent choice understanding the duration of effect is typically in the 1-2 hour range. This effect can be enhanced with N2O-O2. Other drugs that have been administered successfully include zolpidem (Ambien) and zaleplon (Sonata). One challenge with OCS is the ability to titrate making this a less predictable approach than IVCS. Additionally, administering an oral drug sublingually is considered parenteral administration and may require a different permitting level. An approach to consider is administering the drug prior to the appointment, typically prior to sleep, to determine an appropriate effect. The challenge with OCS is not achieving the desired sedation effect. The best approach would be to ensure profound local anesthesia and consider increasing the level of nitrous oxide versus administering additional sedative drug. Ultimately, if OCS is not successful, plan on terminating the appointment and working with your patient to consider other sedation or anesthesia approaches for their procedure.
Anthony Charles Caputo, D.D.S., M.A., F.A.C.D., F.I.C.D., D.A.D.B.A., D.N.D.B.A, is dentist anesthesiologist and president, Southwest Dental Anesthesia Services. He is also a Fellow, American College of Dentists; Fellow, International College of Dentists; Diplomat, American Dental Board of Anesthesiology; and Diplomat, National Dental Board of Anesthesiology. He can be reached at anthony@swdas.com.
[i] Anesth Prog 1990, 36:219-228 Matsuura H. Analysis of systemic complications and deaths during dental treatment in Japan.
[ii] http://time.com/5269371/americans-anxiety-poll/
[iii] https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemNumber=576#Pain