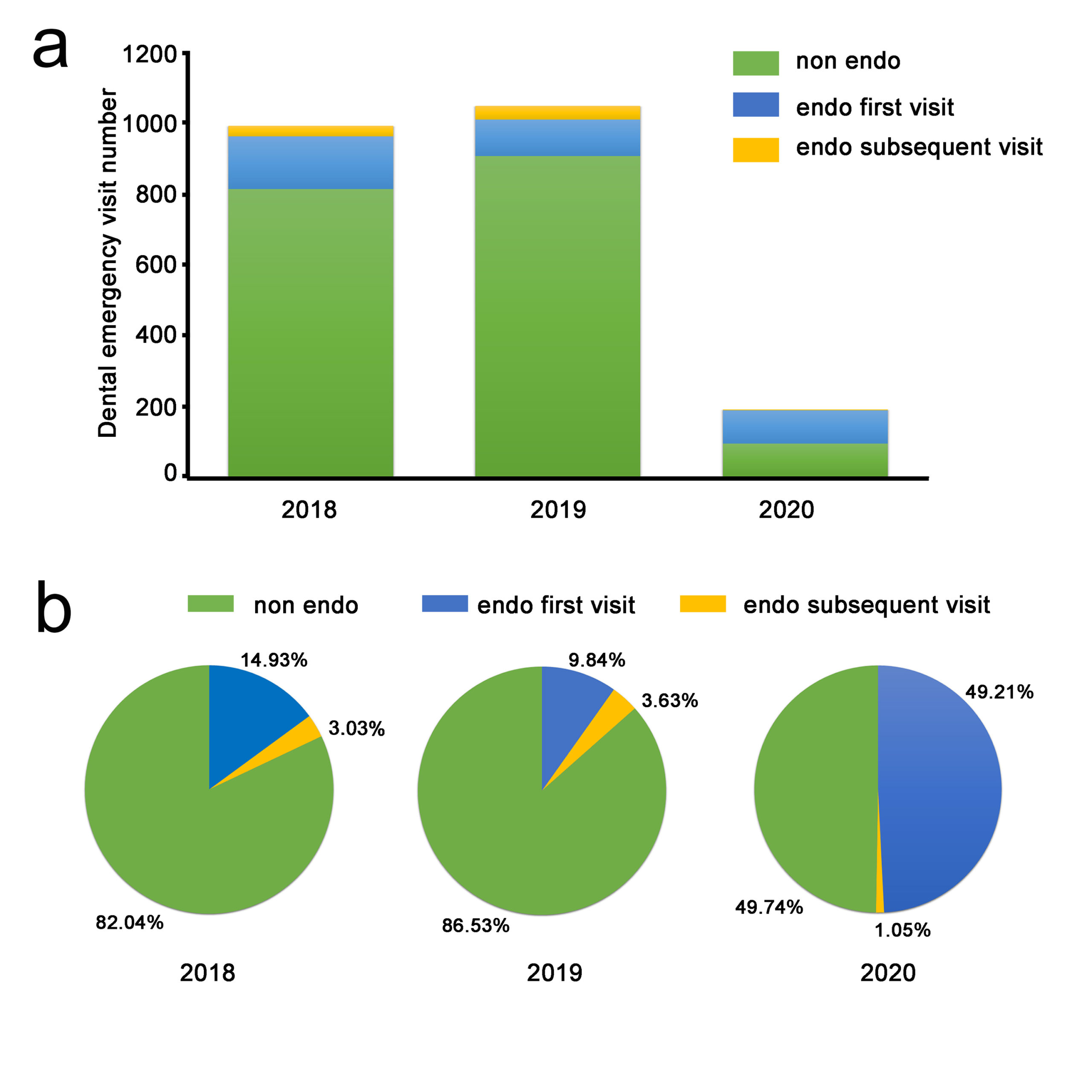
The total number of patients attending General and Emergency Department at WHUSS during the COVID-19 outbreak (n=191) in our study was 18.24% of that of corresponding periods in 2019 (n=1047) and 19.27% of that in 2018 (n=991). These results are consistent with that of a previous study9 that examined patient visits at the Prince Philip Dental Hospital in Hong Kong 10 working days after the severe acute respiratory syndrome (SARS) outbreak in 2003, during which visits dropped to less than one-fifth. The percentage of endodontic emergency patients has increased from 13.47% in 2019, and 17.96% in 2018, to 50.26% during the COVID-19 outbreak in the study. This observed increase could be accounted for by the closing of other facilities that were available to treat endodontic patients under normal operations and possibly by the reduction of trauma as an indirect result of the lockdown. Reduction of outdoor activities by the lockdown may consequently result in a decrease in trauma occurrences, which was reportedly the chief complaint among patients who visited the dental emergency room of a dental hospital in Korea10. These results highlight patient needs for endodontic treatment even under public health emergencies.
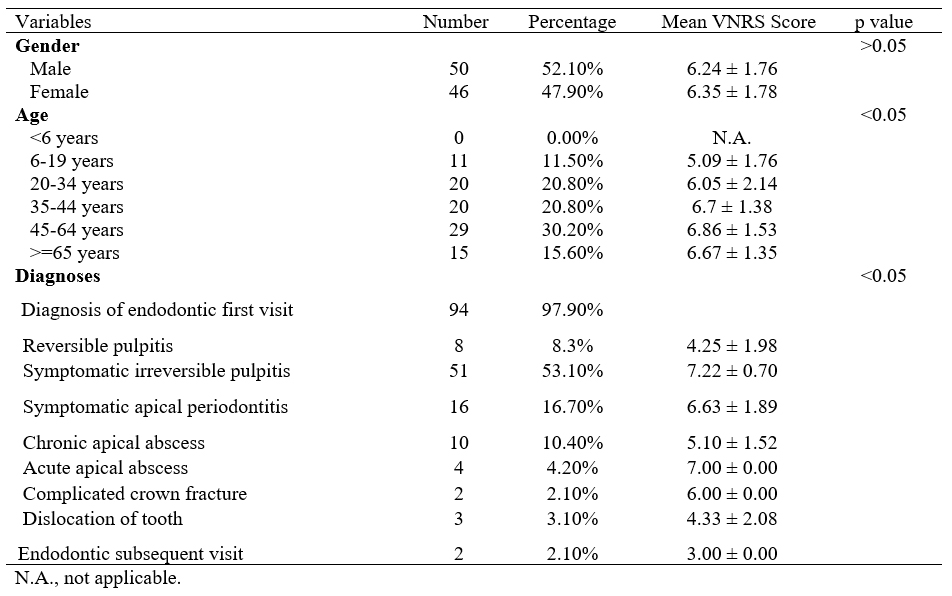
In this study, there was nearly the same ratio of male to female patients for both endodontic emergency patients (1.1:1) and all dental emergency patients (1.2:1), in contrast to other studies11-15 that have shown a greater percentage of male patients presenting with dental emergencies. However, this discrepancy may be due to the higher proportion of endodontic emergency patients in our patient population. The largest age group for endodontic emergencies was 45-64 years (30.21%, 29/96) in our study. Importantly, older age and the existence of underlying comorbidities are associated with poorer COVID-19 prognosis4, 16, 17. Since patients older than 65 years represented approximately 15% of all patients, care should be exercised to avoid cross contamination.
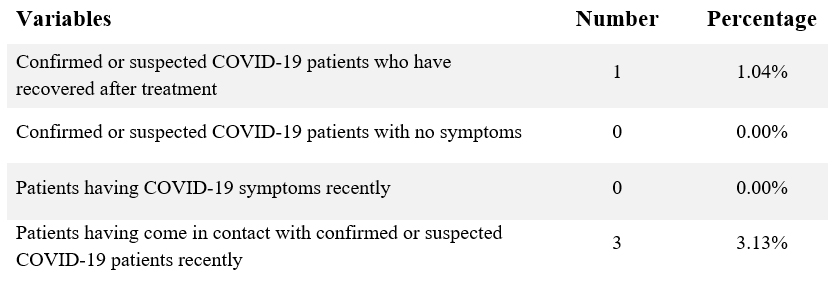
Patient screening was crucial during the SARS epidemic in 2002 and 200318. An important tool in patient screening is the use of disease-specific questionnaires, which can differ depending on the location at which they are employed, for example, epicenter versus other sites. In this study, four patients with a previous COVID-19 history or possible COVID-19 cases were identified using the questionnaire. Fever was reported to be the most common clinical symptom (98%) for 41 patients diagnosed with COVID-19 in a previous study19. No patient with fever presented to the WHUSS due to endodontic emergencies”. Conversely, a patient with pyogenic osteomyelitis of the jaw was found to have fever (>37.2℃), but tested negative for COVID-19 by a series of diagnostic tests. Notably, several infections of the oral cavity could present with fever that could confound the diagnosis of COVID-19; thus fever alone should not be the only sign and symptom of COVID-19 to be evaluated and oral disease needs to be accurately diagnosed. The diagnosis of COVID-19 is currently based on a combination of epidemiologic information, clinical symptoms, chest CT imaging findings, and laboratory tests such as on RT-PCR respiratory tract specimens4. Sabino-Silva et al.20 has raised important questions about the role saliva plays in the human-to-human transmission of diseases, in particular respiratory coronaviruses21, 22.
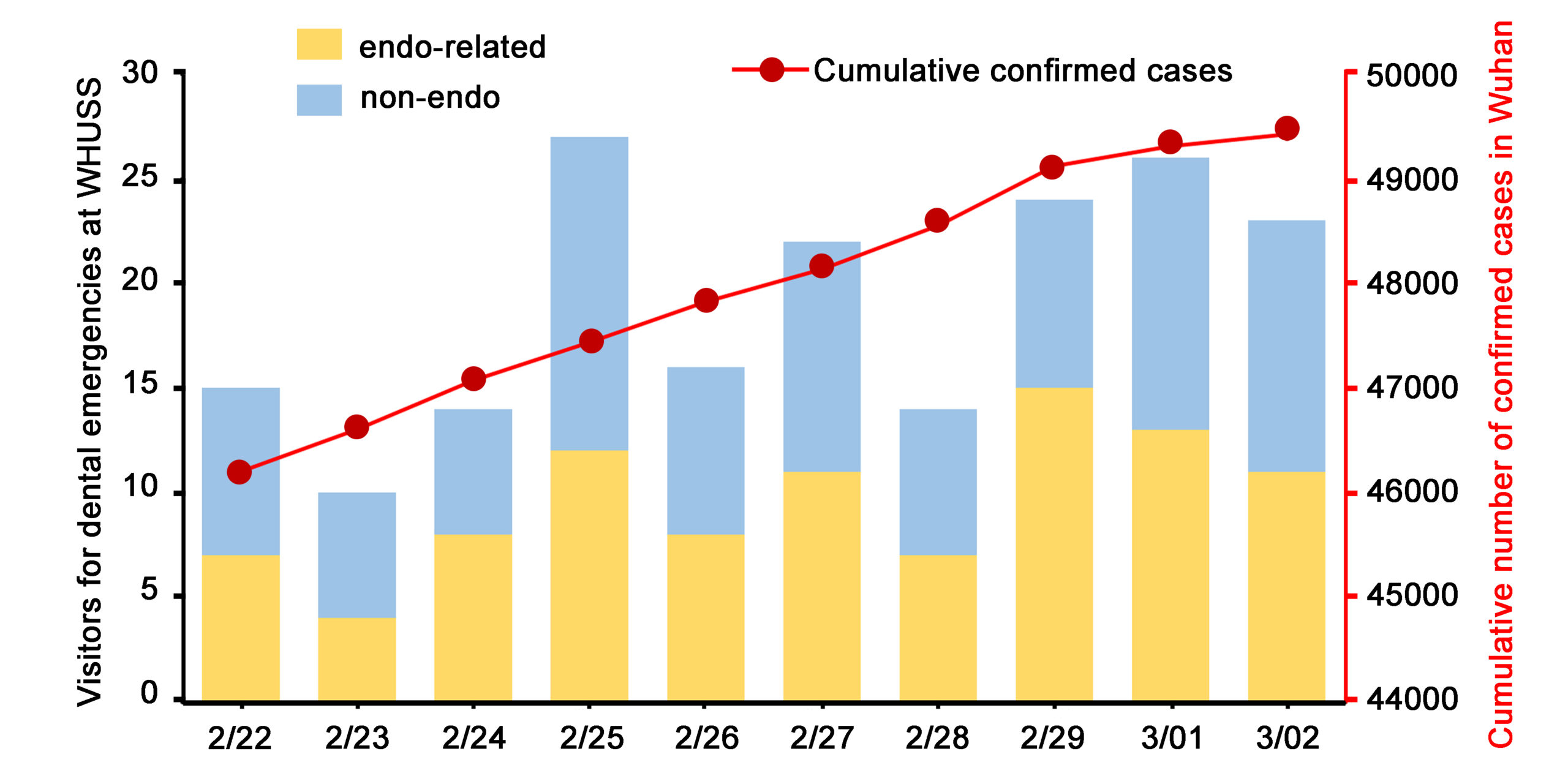
The incubation period of COVID-19 has been estimated to be between 2 to 14 days5. It has been shown that patients with no symptoms or during incubation periods may have the potential to infect others5. Positive RT-PCR test results have been reported in recovered patients23. Endodontists should take appropriate measures to stay safe. During the COVID-19 outbreak, dentists in WUHSS were equipped with disposable N95 masks, gloves, cap, shoe cover, face shield, and gowns4. From February 22, 2020, patients with fever, or who had answered “yes” to any of four questions on the questionnaire, or needing dental procedures producing droplets and/or aerosols were required to undergo examination and treatment in an isolated clinic room with dentists equipped with protective suit instead of gowns4. To date, no cases of COVID-19 were reported among the twenty-six working staff of the General and Emergency Department at WHUSS working during the COVID-19 outbreak. RT-PCR findings for all working staff came back negative on March 24, 2020. Before the beginning of the study, nine working staff at the hospital level have been confirmed to have COVID-19, including three doctors, three nurses, two administrative staff, and one postgraduate student4. This suggests that the safety precautions and screening measures enforced since February 22, 2020, were effective in protecting working staff.
Symptomatic irreversible pulpitis was the most common endodontic emergency, with significant high VNRS score in our study. Treatments for endodontic emergency were challenging during the COVID-19 outbreak, since inhalation of airborne particles and aerosols produced during dental procedures on patients with COVID-19 could potentially expose dentists to the virus20, thus making them high-risk procedures. Reducing treatment time and exposure control are two ways the risk of infection for endodontic treatment could be reduced. For vital pulp cases such as pulpitis, vital pulp therapy including pulpotomy or pulp capping might be helpful in terms of shortening treatment time. Pulpotomy has been reported to reduce pain symptoms in nearly 90% of dental emergency patients 1 day after treatment24. Partial pulpotomy using mineral trioxide aggregate (MTA) sustained a good success rate (85%) over 3-year follow-ups in mature permanent teeth clinically diagnosed with irreversible pulpitis25 and full pulpotomy using MTA demonstrated 92.7% success rate at 3-year follow-up for caries exposed pulps in mature permanent molar teeth26. Direct pulp capping with MTA showed a cumulative survival rate of 85% in adult molars with carious pulpal exposure at 36 months27. For cases that required root canal treatments, cone-beam computed tomography (CBCT) and single file systems should be considered. Besides the advantages of detecting root canal location and configuration28, CBCT examination could avoid nausea or vomiting for patients that may occur during intraoral x-ray examination and prevent exposure to patients’ oral cavity4. During root canal preparation, single file nickel-titanium systems could be used to save working time29, as well as prevent the risk of re-sterilization. For any treatment that produces droplets and/or aerosols, Dr. Hargreaves’ group30 suggested a number of preventative measures, such as the use of rubber dams. It has been reported that up to 70% airborne particles could be reduced around a 3-foot diameter of the operational field when a rubber dam was used31. In addition, rubber dam is not only able to limit the diffusion of the aerosol, but is also likely to dramatically reduce or even eliminate the presence of salivary components in the aerosol.
Only five cases of traumatic dental injury including two cases of “complicated crown fracture” and three cases of “dislocation of tooth,” respectively, were diagnosed in our study. Two patients made a subsequent visit for the completion of their root canal treatments. An online platform for patient consultations by the WHUSS was made available starting February 3, 20204. It was reported that more than 1,600 patients had used this consultation platform, and only dental emergency cases were suggested for treatment at the hospital4.
In addition to providing endodontic treatment, endodontists should pay attention to patients’ psychological health during the COVID-19 outbreak32. Public health emergencies may negatively impact individuals’ mental health33. For instance, one patient in our study had a diagnosis of reversible pulpitis with dentin hypersensitivity had a high VNRS score of 8. She demonstrated extreme anxiety and fear toward gaining a fever as a result of oral disease inflammation. During COVID-19 outbreak period, patients may suffer from psychological stress, endodontists should not only focus on the treatments of patients’ endodontic diseases, but also their psychological state at times of emergency.
In conclusion, endodontic emergencies consist of a much higher portion of dental emergencies in a COVID-19 high risk area than normally. Reducing treatment time and exposure control are two ways to significantly reduce the risk of SARS-CoV-2 virus spreading during endodontic treatment. Vital pulp therapy has the advantage of shortening the treatment time. Rubber dam, personal protective equipment and patient screening are of great importance during the COVID-19 outbreak in protecting clinicians. Dentists should focus not only on the dental treatment but also patients’ psychological status during public health emergencies.