



Clear is Kind: Our Responsibility as Educators

By Kent A. McBride D.D.S., M.S.
What do the following cases have in common?
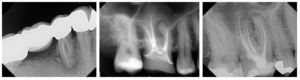
Yes, all three previously treated teeth are great candidates for non-surgical retreatment, but the similarities don’t end there.
All three patients wanted a second opinion because their general dentists gave their teeth hopeless prognoses and suggested expensive implant or FPD treatment plans. Interestingly, these patients self-referred to our office because of positive past experiences.
Now, we’ve all seen patients like these. So the question is, how many similar cases are we NOT seeing because they’ve gone ahead with potentially excessive initial recommendations?
I do believe the vast majority of general dentists sincerely desire to provide the best care for their patients and are not primarily motivated by finances.
But endodontists who have been in practice for any length of time will surely concur that many of our referring doctors lack a deeper understanding of topics like antibiotic usage, diagnosis, retreatment/apical surgery indication, cracked/fractured teeth, resorption, pulpal regeneration, etc.
Unfortunately, many dentists receive biased education from well-meaning sales reps, make decisions based on antiquated research, or apply standard practices from when they were trained (perhaps many years ago).
I can certainly appreciate that as a general dentist, it must be incredibly challenging to keep up with advancements in every specialty while perhaps starting a family, running a practice, and attempting to have a social life simultaneously. It’s both a blessing and a curse that we live in a time with such rapid scientific advancements.
Colleagues, it’s our job to educate. The good news is that educating our dental communities has never been easier. Here are a few very actionable and simple ways:
- Make a quick note in your letter back to the dentist: For example, “Mr. Jones mentioned that you placed him on Clindamycin for his abscess (or worse, for his SIP!). I just wanted to ensure you knew that the FDA recently put a black box warning on Clindamycin. Didn’t want you to be open to liability in the future! Here’s a link.”
- When in doubt, pick up the phone and make a call: Even if it’s a difficult conversation, the dentist will respect you for taking the time to help him/her and advocate for their patient. Clear is kind.
- Use social media: This is such an effective method to educate our dental communities and build our practices. The nuances on approaching it would be an article all to itself, but if you’re overwhelmed by the thought, remember that you can delegate the task to a team member or repost some of the great content many of our colleagues are creating (with permission and credit).
- Host a CE event, lunch and learn, or study club: It doesn’t have to be elaborate. A simple hotel ballroom or conference room with drinks and food will suffice. Don’t be afraid to invite the office staff and keep the information very surface-level. This will go a long way in building rapport, trust, and goodwill.
- Send a printed newsletter to your referring offices: Printed media is NOT dead. We used it for 18 months a few years ago, and it was one of the best marketing and educational tools we’ve ever implemented. Include bios on your doctors, case studies, pictures from team events, etc. There are plenty of companies that will do the heavy lifting and take away the administrative burden.
Remember, the AAE has an abundance of content available for our use. We don’t have to create it all ourselves.
Wishing everyone a safe and happy fall season!
Dr. Kent A. McBride is founder, Meridian Dental Specialists, and partner, North American Dental Group.